
Dejan Filipas
Cholera is one of the most prevalent diseases to afflict our species. It has caused seven pandemics since the 19th century, with many of its victims in Latin America. This analysis will explore the 1991 outbreak in Peru, examining how the country’s infrastructure, economy and culture contributed to the rapid spread of the disease.
Cholera is caused by the bacteria Vibrio cholerae. (1) This releases a toxin which affects the intestine’s ability to regulate the uptake of water, with cells “being tricked” (3) into releasing water rather than absorbing it. This then leads to dehydration and possible death.

Cholera’s devastating impact has mostly been due to the way it spreads, through unclean water supplies as well as crops and seafood (mostly raw shellfish). It has therefore been particularly prevalent in tropical climates and in countries with a high reliance on seafood, both of which apply to Peru, whose seafood consumption sector sustains over 200,000 jobs and is valued at over 5bn USD (2).
Paradoxically, cholera is fairly simple to treat, most commonly via Oral Rehydration Therapy. The patient is given a mixture made up of one litre of safe water, six teaspoons of sugar and a half teaspoon of salt (4). More severe cases are given a mixture of antibiotics and IV fluids.
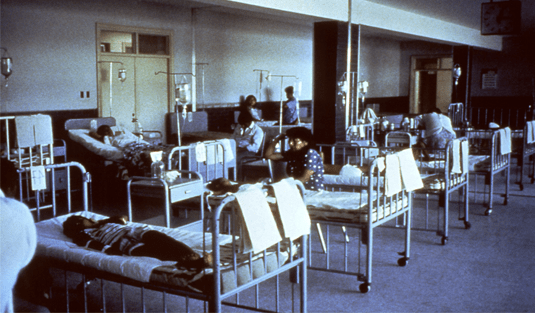
So why was the 1991 epidemic so devastating for Peru specifically, with over 300,000 cases there alone (and another 230,000 elsewhere in the southern hemisphere)? (0)

According to a survey conducted by RE Quick, the combination of tropical weather, a high reliance on seafood and the overall macroeconomic environment led to 75% of respondents drinking untreated water and 91% eating unwashed produce (5).
Moreover, under President Alan García Pérez, the country was in an increasingly difficult economic position, with García limiting the payment of Peru’s debt to the IMF (International Monetary Fund) to only 10% of exports, a measure that directly went against recommendations by international organisations (6). This led to Peru’s credit score falling and to hyperinflation (7000%). By 1991 this had brought about a significant decrease in GDP per capita (8), with inflation being the highest in the region.
All of this resulted in public spending cuts, especially in the social and healthcare sectors, with the latter only receiving a quarter of what it had been allocated in 1980 (7).
This was exacerbated by poor sanitation infrastructure in both urban and rural areas, with Lima (the capital, where the epidemic started) struggling with an aging sewage treatment system. Areas such as Trujillo (on the Pacific north coast) and Iquitos (in the Amazon) had no or very little chlorination, leading to high rates of infection. Over 16,000 cases of cholera were reported in Trujillo (11), with many more probably unreported.
Infrastructure remains a challenge for Peru even today, with 3 million people in Lima not having access to clean, running water and 5 million people not having access to a working toilet. In rural areas almost 20% of the population are still without access to adequate sanitation (12).
It is not surprising therefore that the virus spread to such a large extent, given that the bacteria Vibrio cholarea can be transmitted through contact with infected faeces. The unchlorinated water supply, contaminated with raw sewage, further contributed to the bacteria spreading.
Other hypotheses have been proposed, such as cargo ships bringing cholera, or a connection to El Niño (the cyclical weather phenomenon that heats the ocean near the Peruvian coast). However, it is clear that these are incomplete explanations that can not account for the widespread epidemic at different points in the country.

In conclusion, the evidence points to this epidemic being caused by the systematic failure of government to ensure that appropriate provisions, resources and practices were in place. Peru in 1991 lacked the necessary infrastructure to ensure that its citizens could remain healthy and that any bacterial infection could be contained at a small, endemic level. Contamination of the food chain increased Peruvians’ vulnerability to the disease, with their high reliance on crops and seafood cultivated in water infected by the cholera bacteria.
